
The AUDIT is a 12 question self-report screening questionnaire designed to measure harmful alcohol use. This includes the 10 standard questions of the AUDIT and this version includes 2 optional questions at the end to determine self-identified problem drinking and self-perceived difficulty in stopping drinking.
The AUDIT is widely used and useful for routine screening in community health settings and was developed in conjunction with the World Health Organisation.
It is sensitive to three factors of problematic alcohol use:
The AUDIT differs from other self-report screening tests in that it was based on data collected from a large multinational sample, used a statistical rationale for item selection, emphasises identification of hazardous drinking rather than long-term dependence and adverse drinking consequences, and focuses primarily on symptoms occurring during the recent past rather than “ever”.
Total scores range from 0 to 40, with higher scores indicating greater likelihood of hazardous and harmful drinking. Scores are also presented as a percentile compared to a sample of individuals enrolled in a drink driving treatment program (Hays & Merz, 1995). A percentile of 50 indicates a typical score for someone with serious drinking related driving offences, with higher percentiles indicate high severity. Percentiles below 30 likely indicate no drinking problem.
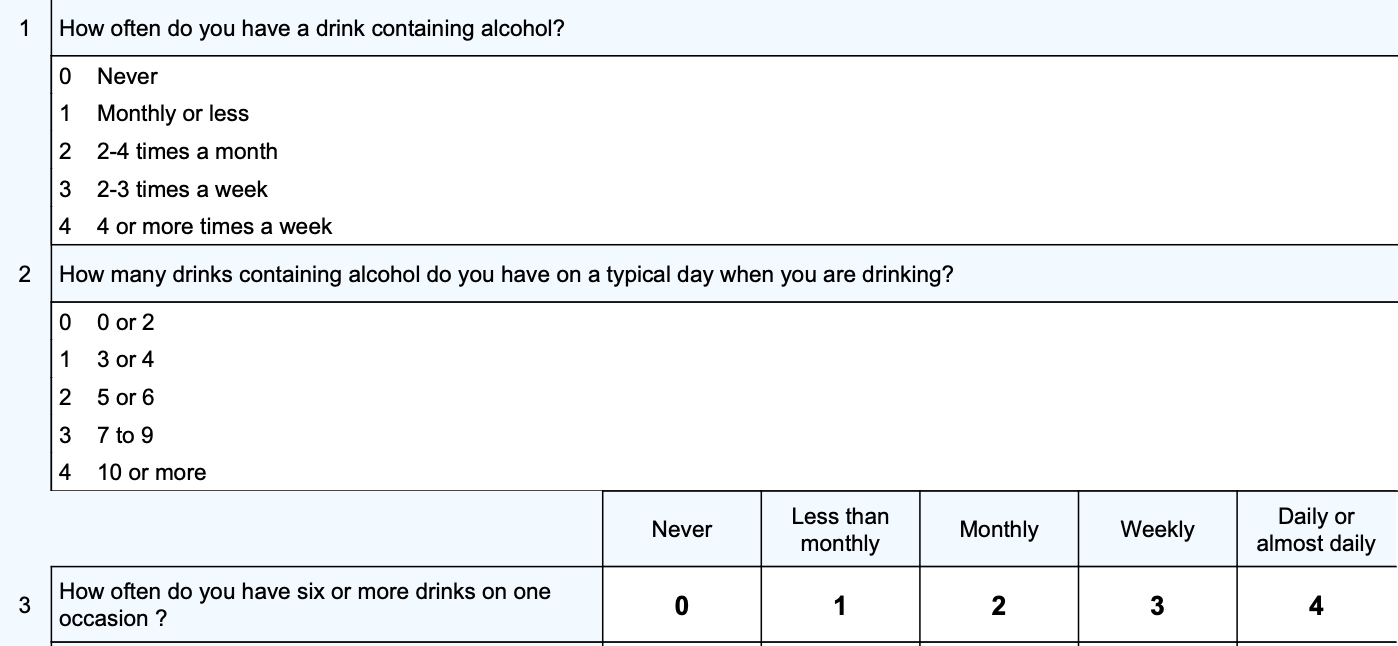
Scoring is computed by adding scores (0 – 4) on questions 1 to 8, and questions 9 and 10 scored 0, 2, or 4 points. Questions 11 and 12 are not scored.
Risk levels are presented based upon the following total scores:
Total scores of 8 or more are recommended as indicators of hazardous and harmful alcohol use. However, a score of 8 or more will only be sensitive to 59% of individuals who actually have drinking problems, (Bush et al, 1998). Therefore, scores should only be used as an indication of alcohol problems and not to definitively rule it out.
When looking at individual responses the questions can be conceptualised using the following three categories:
A raw score above 4 (standard score 3.3) on the Dependence subscale indicates that the client may have alcohol dependency. If a client scores of 4 or more then it is recommended that further assessment be completed to determine if dependence is confirmed.
The last two questions help with managing self-beliefs about drinking problems and self-perceived difficulties in stopping or reducing drinking levels within the next 3 months.
Psychometric PropertiesIn the test development sample (Saunders et al, 1993), a cut-off value of 8 yielded sensitivities for various indices of problematic drinking that were in the mid 0.90s.
Subsequent research has evaluated the AUDIT against other measures of alcohol problems including data from comprehensive interviews. One such study (Bush, et al, 1998) found that among 477 participants who completed the AUDIT and were interviewed to determine significant alcohol related problems, a cutoff score of 8 had a sensitively (false negative) of 59% and a specificity (false positive) of 91%. That is, a score of 8 or more will only be sensitive to 59% of individuals who actually have drinking problems, and one can be 91% sure it is not a false positive.
Hays and Merz (1995) gave 832 individuals who were enrolled in drink driving treatment program in California the AUDIT and found that the average score was 8.6 (SD 6.9). This data is used to compute percentiles but given the positive skew should be interpreted with caution.
Professional Access
Saunders, J.B., Aasland, O.G., Babor, T.F., de la Fuente, J.R. and Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption. II. Addiction, 88, 791-804,
1993.
Saunders, J.B., Aasland, O.G., Amundsen, A. and Grant, M. Alcohol consumption and related problems among primary health care patients: WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption I. Addiction, 88, 349-362, 1993.
Miller, W.R., Zweben, A., DiClemente, C.C. and Rychtarik, R.G. Motivational enhancement therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. Project MATCH Monograph Series, Vol. 2. Rockville MD: NIAAA, 1992.
Bush, K., Kivlahan, D., Mcdonell, M., Pihn, S., Bradley, K., The AUDIT Alcohol Consumption Questions (AUDIT-C): An Effective Brief Screening Test for Problem Drinking, Arch Intern Med, 1998;158(16):1789-1795
Hays, R., Merz, J., Response burden, reliability, and validity of the Cage, Short MAST, and AUDIT alcohol screening measures, Behavior Research Methods, Instruments, & Computers, 1995, 27 (2), 277-280.